Every few months, a new vendor promises a “zero touch” clinical coding automation pipeline: feed in raw text, let the algorithm match it against MedDRA coding or the WHO Drug Dictionary, and watch the manual work disappear.
It’s a clean pitch. Real trial data just doesn’t cooperate with it.
Data pulled from CRFs, investigator notes, and SAE narratives across multi-center, multi-country studies is inherently messy. Even well-built sequential pipelines still route a meaningful share of records to human review, and the reasons are consistent. Industry benchmarks make this concrete: a peer-reviewed evaluation of WHODrug Koda published in Drug Safety (Meldau et al., 2022) found that, compared with a simple direct-match baseline, AI-powered medical coding could raise automation from 61% to 89% while maintaining 97% coding accuracy.
Even with one of the more advanced engines published in the literature, roughly 1 in 10 records still need a human, and simpler matching approaches can leave as many as 4 in 10 unautomated. Automation tends to fail in three predictable places, each one harder to solve than the last.
Here is a look behind the curtain at why automation hits a wall, and why expert medical coders remain completely irreplaceable:
1. The Garbage-In, Garbage-Out Ingestion Dilemma
An algorithm can only act on the text it’s given, and source data is full of small failures that break naive logic before coding even begins:
- Blank or near-blank fields. A verbatim entry that’s empty, or just a stray space, has to be rejected outright. Otherwise, the system risks creating phantom entries.
- The isolated modifier trap. A field containing only “500mg” or “BID” gives the engine nothing to look up. Flip it around, “aspirin 100mg,” and now it needs real parsing logic just to strip the dose and rescue the drug name.
- Text contamination. Stray HTML, nested punctuation, and special characters appear frequently. Some are safe to drop; others, like +, /, and &, carry structural meaning under UMC guidelines and must survive cleanup intact.
This is the easy layer, relatively speaking, fixable with better parsing rules. The next layer isn’t.
2. The Semantic “Me Too” Trap and Fuzzy Matching Failures
Many automated models rely heavily on string similarity metrics, such as the Levenshtein distance. While this works well for simple typos, it introduces significant risks when processing closely related clinical formulations.
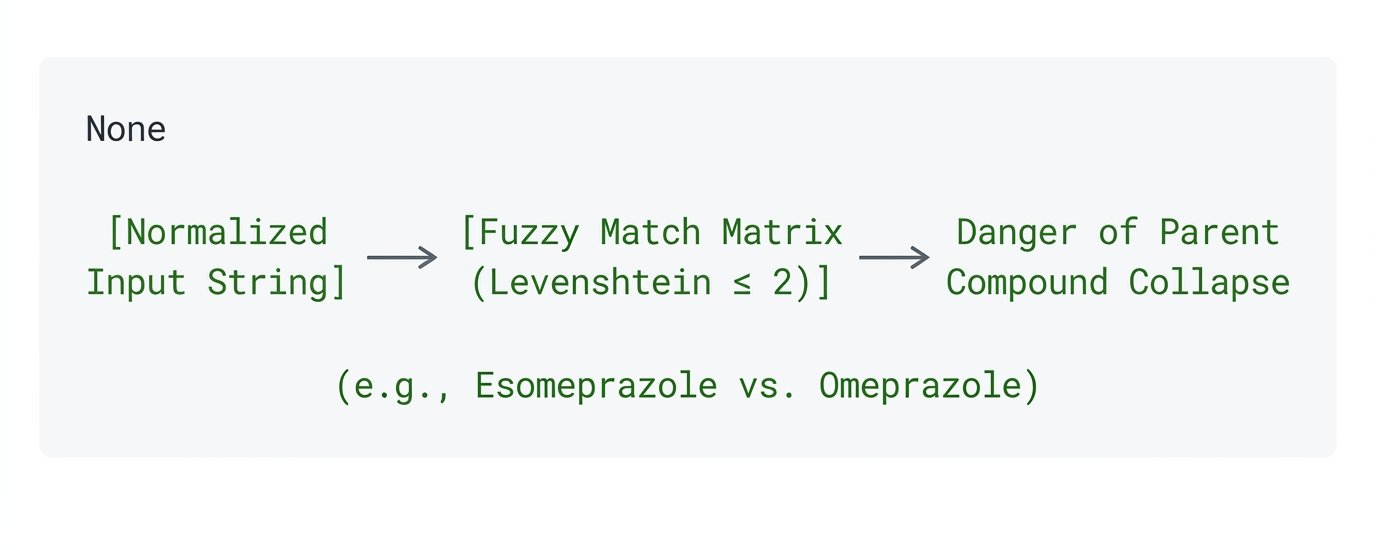
In the pharmaceutical world, a single letter can alter a drug’s entire pharmacodynamic profile. For instance, “me-too” variations or mirror-image stereoisomers like esomeprazole and omeprazole are distinct therapeutic compounds. If an auto-encoder relies on fuzzy string matching, it may inadvertently auto-correct a newer compound to its more common parent drug.
It compounds from there. Coders can’t flatten everything to the generic active ingredient; they have to preserve the verbatim brand Drug Record Number to protect market authorization traceability. And some brand names map to different INNs depending on the country (Crocin is the classic case). When that happens, there’s no safe default. The system has to stop and defer to someone who knows the market.
No amount of tuning the matching threshold fixes this. It requires judgment, not precision.
3. The Multi-ATC Riddle: Disambiguation Requires Context
This is where most manual escalation actually comes from. A drug like aspirin or ketoconazole doesn’t have one ATC code; it has several, depending entirely on why and how it was used.
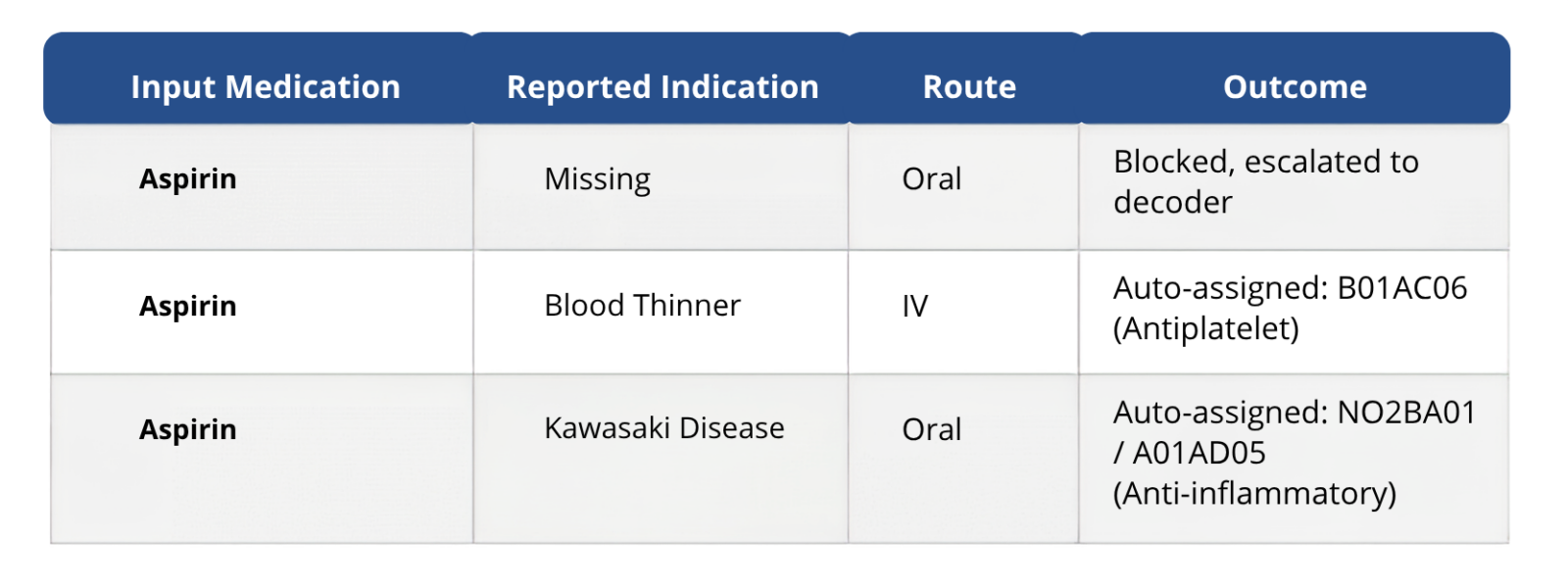
An algorithm can’t infer clinical intent from a blank indication field, and it shouldn’t try to. When context is missing, the correct move is to stop, flag it (ATC_AMBIGUOUS_NO_INDICATION), and let a human make the call.
How AI and Coders Work Together
The most effective medical coding workflow isn’t AI replacing coders or coders ignoring AI. It’s a clean handoff: AI clears the records it can code with confidence, and routes the rest, ambiguous indications, conflicting brand names, and multi-ATC drugs straight to a human who has the context to resolve them. The system’s job is to know which bucket each record belongs in, not to guess its way through the hard ones.
How Smart Medical Coding Improves Clinical Coding
This is the gap Smart Medical Coding (SMC), our medical coding solution, is built around. Instead of promising to remove coders from the loop, SMC is designed for the reality above: AI-assisted medical coding clears the volume, and people handle the judgment calls, with the system actively flagging which is which.
Benefits of AI-Assisted Medical Coding
- AI-powered coding acceleration. NLP-driven MedDRA and WHODrug suggestions with confidence scoring, so coders start from a ranked shortlist, not a blank dictionary search.
- Built-in escalation logic. Missing indications, conflicting INNs, and multi-ATC drugs route automatically to review instead of getting force-coded.
- Continuous learning. Every reviewer decision feeds back into the model, so the system gets sharper instead of repeating the same fuzzy-match mistakes.
- Audit-ready governance. Full 21 CFR Part 11 traceability on every coding decision, automated or human.
Conclusion
This is a case for being honest about what automation is actually good at. Clean, unambiguous records, the bulk of any study’s coding volume, can and should move through a pipeline without a human ever touching them. The remaining cases, the blank fields, the near-duplicate drug names, and the multi-ATC ambiguity aren’t failures of the technology. They’re exactly the records that were always going to need a person.
The teams that get the most out of coding automation aren’t the ones chasing a 100% auto-coding rate. They’re the ones who’ve built a system that knows the difference between the two, so coders spend their time on the records that actually need their expertise, instead of the ones that never should have reached them in the first place.
If your team is still spending hours a week untangling exactly these three problems, it’s worth seeing how SMC handles them in practice. Request a demo to walk through it on your own coding data.
FAQs
Q1. What are the benefits of AI-powered medical coding?
A. AI-powered medical coding speeds up coding cycles, improves consistency across studies, reduces manual dictionary searching, and gives coders ranked, confidence-scored suggestions instead of a blank search. It also strengthens audit readiness through built-in traceability, while keeping human review on the records that genuinely need judgment.
Q2. What is automated medical coding?
A. Automated medical coding uses NLP and dictionary-matching algorithms to map verbatim terms from clinical trial data, like adverse events or concomitant medications, to standardized codes in dictionaries such as MedDRA and WHODrug, with minimal manual intervention for straightforward, unambiguous records.
Q3. Can medical coding be fully automated?
A. Not entirely, and that’s by design. Even advanced AI coding engines still route a portion of records, those with missing context, conflicting drug names, or multi-ATC ambiguity, to human coders. Published benchmarks show top-performing engines can reach up to 89% automation, but the remaining records require expert judgment that automation shouldn’t attempt to replace.
Q4. What is MedDRA coding?
A. MedDRA (the Medical Dictionary for Regulatory Activities) coding is the process of mapping verbatim terms, such as reported adverse events or medical history, to standardized MedDRA terminology. It ensures consistent, regulatory-compliant terminology across clinical trials and safety reporting.
Q5. How does Smart Medical Coding improve efficiency?
A. Smart Medical Coding combines AI-powered coding suggestions, automated escalation logic, peer review workflows, and dictionary lifecycle management in a single platform. This reduces manual dictionary searching, speeds up coding turnaround, and improves consistency across studies, while keeping human coders focused only on the records that require their expertise.
