Ask any clinical operations leader where study startup time disappears, and the answer rarely points to a single dramatic failure. More often, the culprit is a slow, grinding process that most teams simply accept as unavoidable: building the Electronic Data Capture (EDC) system.
Between protocol finalization and the first patient visit, skilled data managers are forced to hand-translate clinical intent into technical configurations. This “translation” period is quietly one of the most expensive bottlenecks in modern clinical trials, and it starts much deeper than most organizations realize.
The Interpretive Gap: From Protocol to EDC
A finalized protocol is a dense, layered document. Converting it into an accurate, validated EDC build requires an expert to work across multiple, often conflicting, data streams:
- Schedule of Activities (SoA): Managing visit windows, timing rules, and the “fine print” in protocol-specific footnotes.
- Eligibility and Dosing Logic: Encoding the criteria that drive form behavior and edit check conditions.
- Lab Thresholds and AE Grading: Ensuring values are encoded precisely to meet safety reporting requirements.
- CDISC Field Mappings: Aligning protocol-specific elements with rigid submission standards.
This requires someone who can read a protocol like a clinician but configure a system like an engineer. Even then, the manual process, such as specification, review, configuration, testing, and rework, is frequently repeated four or five times before a build is signed off.
The Hidden Cost Is Not Just Time
Study startup accounts for 30-40% of total trial duration (Tufts CSDD), and EDC build cycles are among its most persistent contributors. At an estimated cost of $600,000 to $8 million per day of Phase III delay, depending on the asset, the stakes of a slow or error-prone build are difficult to overstate. The compounding effects are worse than most teams account for:
- Delayed site activation stalls enrollment before it begins
- Over-engineered edit checks generate query churn that burdens sites and erodes trust
- Under-specified validations allow dirty data to accumulate throughout the life of the study
- Mapping gaps surface during submission preparation, at exactly the wrong moment
The industry has largely normalized this. It shouldn’t.
Why Amendments Compound the Problem
If initial build cycles are painful, mid-study amendments are acute. A change to an eligibility criterion or a modified visit schedule triggers a cascade of EDC consequences.
Today, that impact assessment is largely a manual audit. A data manager must read the amendment, compare it to the current build, and determine the “ripple effect.” It is painstaking work where a single missed field can lead to significant downtime or data integrity issues later in the trial.
Why Agentic AI Changes the Model
Most AI in clinical data management has been purely assistive- helpful for flagging an anomaly or surfacing a recommendation, but limited. The AI points to a problem, and the human still has to do the heavy lifting to fix it.
Agentic AI works differently. It doesn’t just suggest; it executes.
- It acts instead of waiting. Rather than waiting for a prompt, it reads and reasons through the full complexity of a protocol to complete a task from start to finish.
- It connects the dots. It simultaneously processes the protocol narrative, SoA, form libraries, and CDISC standards (details humans usually have to juggle manually).
- It shifts the load to review. Instead of starting with a blank page, the data manager receives a structured, traceable draft. The job moves from “building” to “validating.”
- It produces results. This isn’t a list of suggestions. It is a coherent, standards-aligned build package ready for expert interrogation.
That shift from assistive to agentic is exactly how weeks of startup time are recovered.
A Smarter Starting Point: Saama EDC Study Build & Start-Up
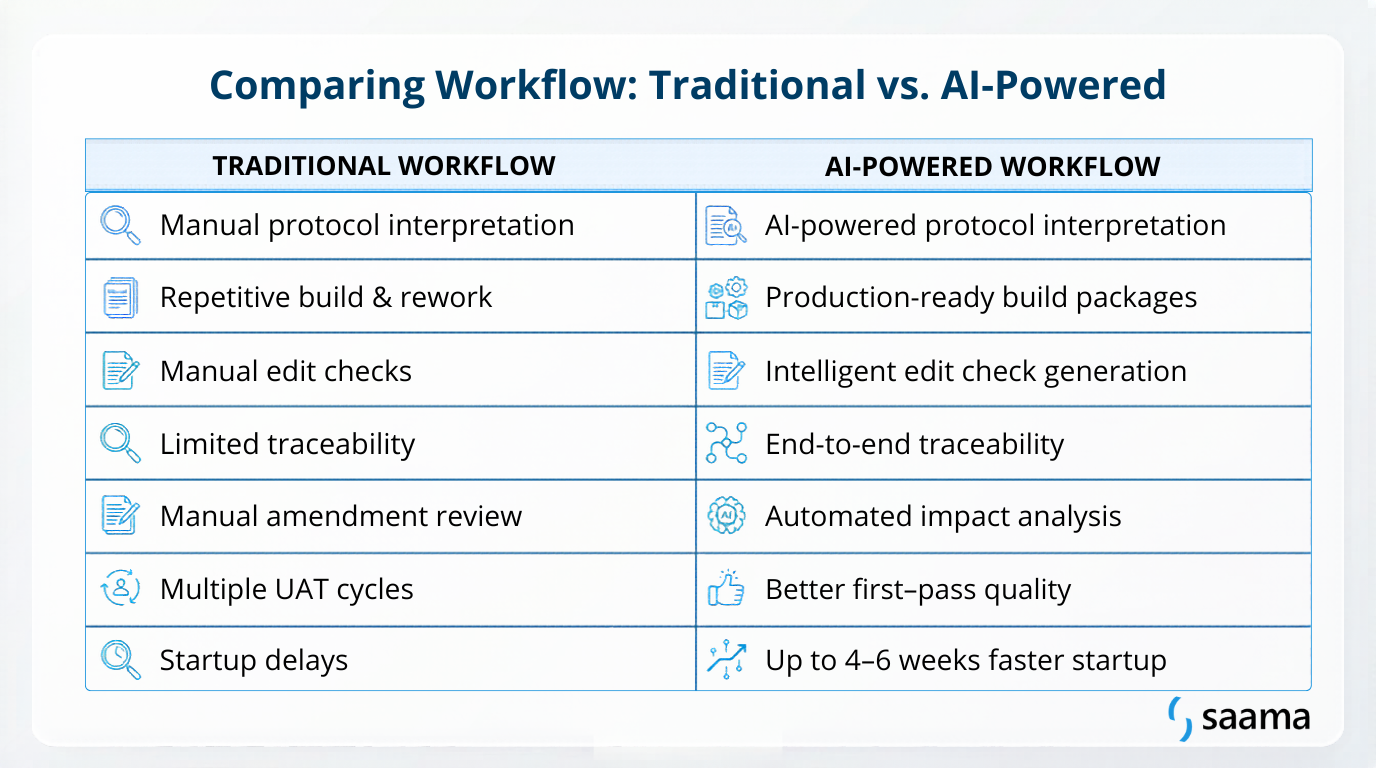
To break this cycle, the industry is moving away from manual specification writing. Saama’s EDC Study Build & Start-Up changes the process’s starting point. Rather than starting from a blank spreadsheet, it applies AI-driven reasoning to interpret the digitized protocol and generate the technical artifacts automatically.
The human remains in control, but the workflow is fundamentally different:
- Standards-Aligned Recommendations: The system suggests forms and fields mapped to CDISC and organizational libraries, ensuring 1:1 traceability back to the protocol.
- Intelligent Edit Check Generation: Logic is grounded in the actual protocol footnotes and visit windows, capturing what is needed without creating “noisy” data environments.
- Validation Test Case Creation: Automated scenarios verify form behavior and logic before User Acceptance Testing (UAT) even starts.
- Amendment Impact Packages: Structured analysis that tells you exactly what changed and what needs re-validation, cutting down on amendment-related downtime.
Getting Ahead of the Schedule
Weeks lost to EDC build cycles are weeks your sites are not enrolling, and your timelines are slipping. By moving from manual entry to AI-accelerated configuration, teams are reclaiming that lost month.
Data managers are not replaced in this model; they are elevated. By removing the mechanical “grunt work” of specification writing, they can focus on high-level clinical judgment and data strategy. The result is a higher-quality build on the first pass and a trial ready to run from Day One.
If you are ready to see what a faster, smarter EDC build looks like in practice, reach out to us at [email protected].
